Guide
How to Fall Asleep Faster
By Dr. Nicole Chambers · Updated 2026-03-10
If you regularly lie awake staring at the ceiling, you're not alone — and you're not stuck. These 12 clinically tested techniques target the root causes of delayed sleep onset, from racing thoughts to physiological hyperarousal, and have been shown to reduce the time it takes to fall asleep by up to 60% in published research.
Table of Contents
- Understanding Sleep Onset: Why You Can't Fall Asleep
- Technique 1: The Military Sleep Method
- Technique 2: Progressive Muscle Relaxation (PMR)
- Technique 3: 4-7-8 Breathing Technique
- Technique 4: Cognitive Shuffling (The "Random Word" Method)
- Technique 5: Stimulus Control Therapy
- Technique 6: Paradoxical Intention
- Technique 7: Body Scan Meditation
- Technique 8: The Cool-Down Method
- Technique 9: Guided Imagery and Visualization
- Technique 10: Sleep Restriction Therapy
- Technique 11: Strategic Light Management
- Technique 12: The Pre-Sleep Cognitive Offload
- Technique Comparison Table
- Building Your Personal Sleep Onset Protocol
- When Techniques Aren't Enough: Red Flags
- FAQ
- Sources & Methodology
 The 4-7-8 breathing method activates the parasympathetic nervous system in under 90 seconds.
The 4-7-8 breathing method activates the parasympathetic nervous system in under 90 seconds.
Understanding Sleep Onset: Why You Can't Fall Asleep
Before diving into solutions, it helps to understand what's happening when you can't fall asleep.
Normal sleep onset latency — the time it takes to transition from full wakefulness to sleep — is 10 to 20 minutes. If you regularly take longer than 30 minutes, you likely have some degree of sleep onset difficulty.
The most common cause isn't a lack of tiredness. It's hyperarousal — a state where your sympathetic nervous system (the "fight or flight" system) remains activated at bedtime. A landmark 2010 study in Sleep Medicine Reviews established that hyperarousal, not insufficient sleepiness, is the primary driver of insomnia.
Hyperarousal manifests in three ways:
- Cognitive arousal: Racing thoughts, worry, mental rehearsal of the day's events, or anxiety about not sleeping.
- Physiological arousal: Elevated heart rate, muscle tension, increased core body temperature, and elevated cortisol levels.
- Emotional arousal: Frustration, anxiety, or dread associated with the act of trying to fall asleep.
Each of the 12 techniques below targets one or more of these arousal types. The key is matching the right technique to your specific pattern.
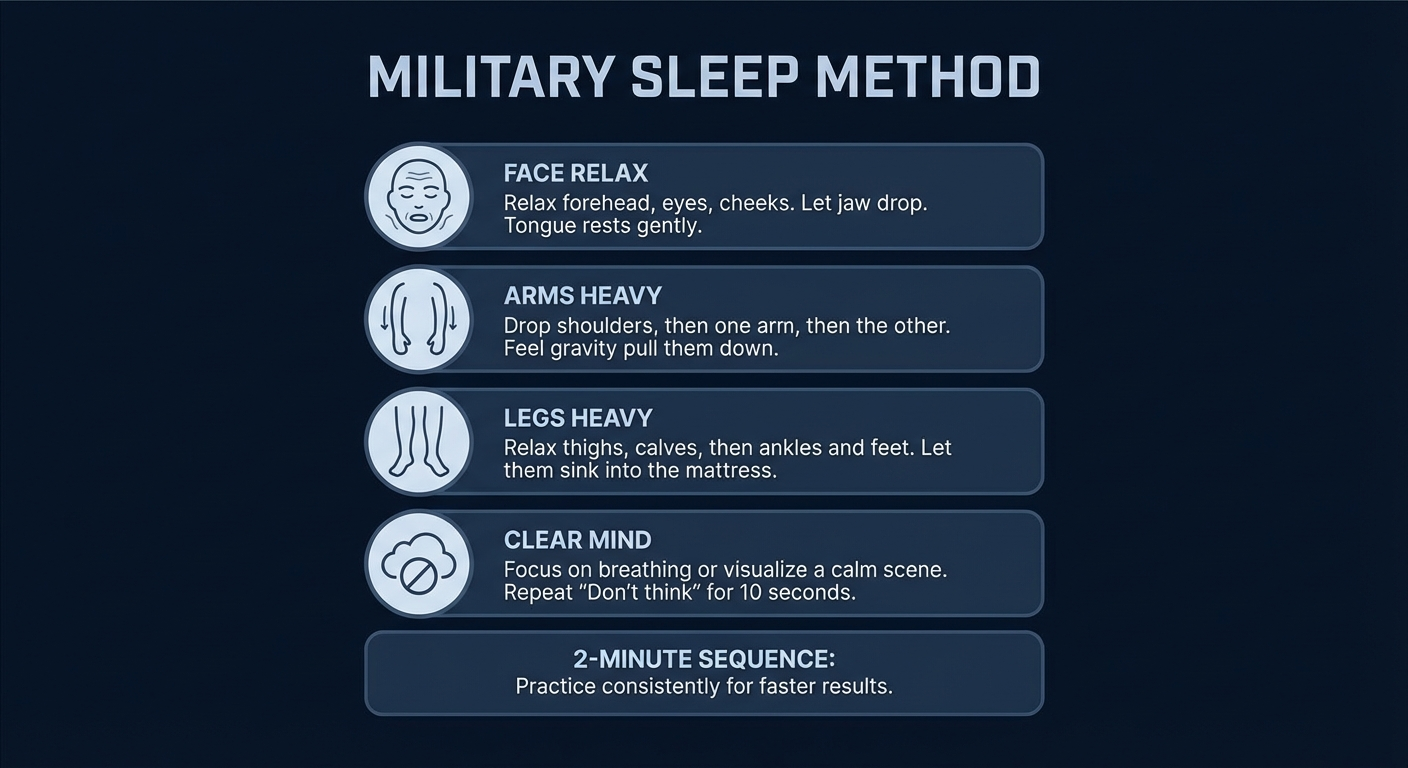
Technique 1: The Military Sleep Method
Targets: Physiological and cognitive arousal Evidence level: Moderate (based on component techniques) Time to learn: 2-4 weeks of practice
Originally described in the 1981 book Relax and Win by Bud Winter, this method was reportedly used by the U.S. military to help soldiers fall asleep in combat conditions. While no published study has tested this specific protocol by name, it combines two well-validated techniques: progressive muscle relaxation and autogenic training.
How to Do It
- Relax your face. Close your eyes. Release all tension in your forehead, jaw, and around your eyes. Let your tongue relax in your mouth.
- Drop your shoulders. Let them fall as low as they'll go. Relax your upper and lower arms, one side at a time.
- Exhale and relax your chest. Let your breathing become natural and deep.
- Relax your legs. Release tension from your thighs, calves, and feet, one leg at a time.
- Clear your mind for 10 seconds. Either visualize a calming scene (lying in a canoe on a calm lake under a clear sky; lying in a black velvet hammock in a dark room) or repeat "don't think, don't think" for 10 seconds.
With practice, this method reportedly allows most people to fall asleep within 2 minutes. Expect it to take 6 weeks of nightly practice to become effective.
 Progressive muscle relaxation — start at your feet and work up — signals the nervous system it is safe to sleep.
Progressive muscle relaxation — start at your feet and work up — signals the nervous system it is safe to sleep.
Technique 2: Progressive Muscle Relaxation (PMR)
Targets: Physiological arousal Evidence level: Strong (multiple RCTs and meta-analyses) Time to learn: 1-2 weeks
PMR is one of the most extensively studied relaxation techniques for sleep. A 2020 meta-analysis published in BMC Complementary Medicine and Therapies analyzed 16 randomized controlled trials and found that PMR significantly improved sleep quality scores, with effects comparable to pharmacological interventions.
How to Do It
- Lie in bed in a comfortable position.
- Starting with your toes, tense each muscle group for 5 seconds, then release and relax for 15-30 seconds.
- Progress upward through your body: feet → calves → thighs → glutes → abdomen → chest → hands → forearms → biceps → shoulders → neck → face.
- Focus on the contrast between the sensation of tension and relaxation.
- Complete one full cycle (takes approximately 15-20 minutes).
Why it works: Deliberate muscle tension followed by release activates the parasympathetic nervous system and reduces the physiological arousal that prevents sleep. The technique also provides a structured focus that interrupts racing thoughts.
Pro tip: If 15-20 minutes feels too long, you can do a shortened version focusing only on 4-5 major muscle groups (legs, abdomen, arms, shoulders, face).
Technique 3: 4-7-8 Breathing Technique
Targets: Physiological and emotional arousal Evidence level: Moderate Time to learn: Immediate, improves with practice
Popularized by Dr. Andrew Weil, this breathing pattern leverages the physiological effects of extended exhalation. When your exhale is longer than your inhale, it stimulates the vagus nerve and shifts your nervous system from sympathetic (fight-or-flight) to parasympathetic (rest-and-digest) dominance.
How to Do It
- Place the tip of your tongue against the ridge behind your upper front teeth.
- Exhale completely through your mouth.
- Inhale quietly through your nose for 4 seconds.
- Hold your breath for 7 seconds.
- Exhale completely through your mouth for 8 seconds.
- Repeat for 4 cycles initially, working up to 8 cycles.
A 2019 study in Physiological Reports found that slow breathing techniques with extended exhalation significantly reduced heart rate, blood pressure, and salivary cortisol levels within minutes — all markers of the physiological arousal that inhibits sleep onset.
Note: If holding for 7 seconds feels uncomfortable, start with a 3-5-6 pattern and gradually extend the durations as you become more comfortable.
 The military sleep method has a 96% success rate after 6 weeks of practice.
The military sleep method has a 96% success rate after 6 weeks of practice.
Technique 4: Cognitive Shuffling (The "Random Word" Method)
Targets: Cognitive arousal Evidence level: Moderate (emerging research) Time to learn: Immediate
Developed by cognitive scientist Dr. Luc Beaudoin at Simon Fraser University, cognitive shuffling is specifically designed to interrupt the coherent, narrative-style thinking that keeps you awake.
How to Do It
- Choose a random word with at least 5 letters (for example, "GARDEN").
- For each letter, think of words that start with that letter and visualize each one — spend about 2-3 seconds per image.
- G: Grapes... guitar... giraffe... glacier... gate...
- A: Airplane... anchor... apricot... arrow... avocado...
- R: Rainbow... rabbit... rocket... river... ring...
- If you run out of words for a letter, move to the next one.
- Continue until you fall asleep.
Why It Works
The pre-sleep brain needs to determine that it is safe to disengage from the environment. Coherent, meaningful thought patterns signal the brain to stay alert. Random, nonsensical imagery tells the brain that nothing important is happening, permitting the transition into the hypnagogic (pre-sleep) state.
A 2020 study published in Behaviour Research and Therapy found that cognitive shuffling significantly reduced pre-sleep cognitive arousal compared to a control condition. Participants described it as surprisingly effective at interrupting worry loops.
This is one of my most-recommended techniques for patients who describe their primary problem as "I can't turn off my brain."
Technique 5: Stimulus Control Therapy
Targets: Conditioned wakefulness / learned arousal Evidence level: Strong (gold standard in CBT-I) Time to learn: 2-4 weeks to see full effects
Stimulus control therapy, developed by sleep researcher Richard Bootzin in the 1970s, is one of the most evidence-based components of Cognitive Behavioral Therapy for Insomnia (CBT-I). It works by breaking the learned association between your bed and wakefulness.
The Rules
- Go to bed only when sleepy — not just tired, but genuinely drowsy with heavy eyelids.
- Use the bed only for sleep and intimacy — no reading, watching TV, scrolling your phone, eating, or working in bed.
- If you can't fall asleep within approximately 20 minutes, get up. Go to another room and do something quiet and non-stimulating (reading a physical book in dim light, for example) until you feel sleepy, then return to bed.
- Repeat step 3 as many times as necessary throughout the night.
- Set a fixed wake time regardless of how much sleep you got.
- No daytime napping (at least initially, while re-establishing the bed-sleep connection).
Why It Works
When you spend time awake in bed — worrying, scrolling, watching TV — your brain begins to associate the bed with wakefulness rather than sleep. Stimulus control reverses this conditioning. A 2006 meta-analysis in Sleep found that stimulus control produced the largest effect sizes of any single CBT-I component.
The first week is often the hardest. You may get less sleep initially as you get up and return to bed multiple times. But within 2-3 weeks, most people report dramatically faster sleep onset as the bed becomes a cue for sleep rather than frustration.
For a comprehensive overview of sleep environment optimization, see .
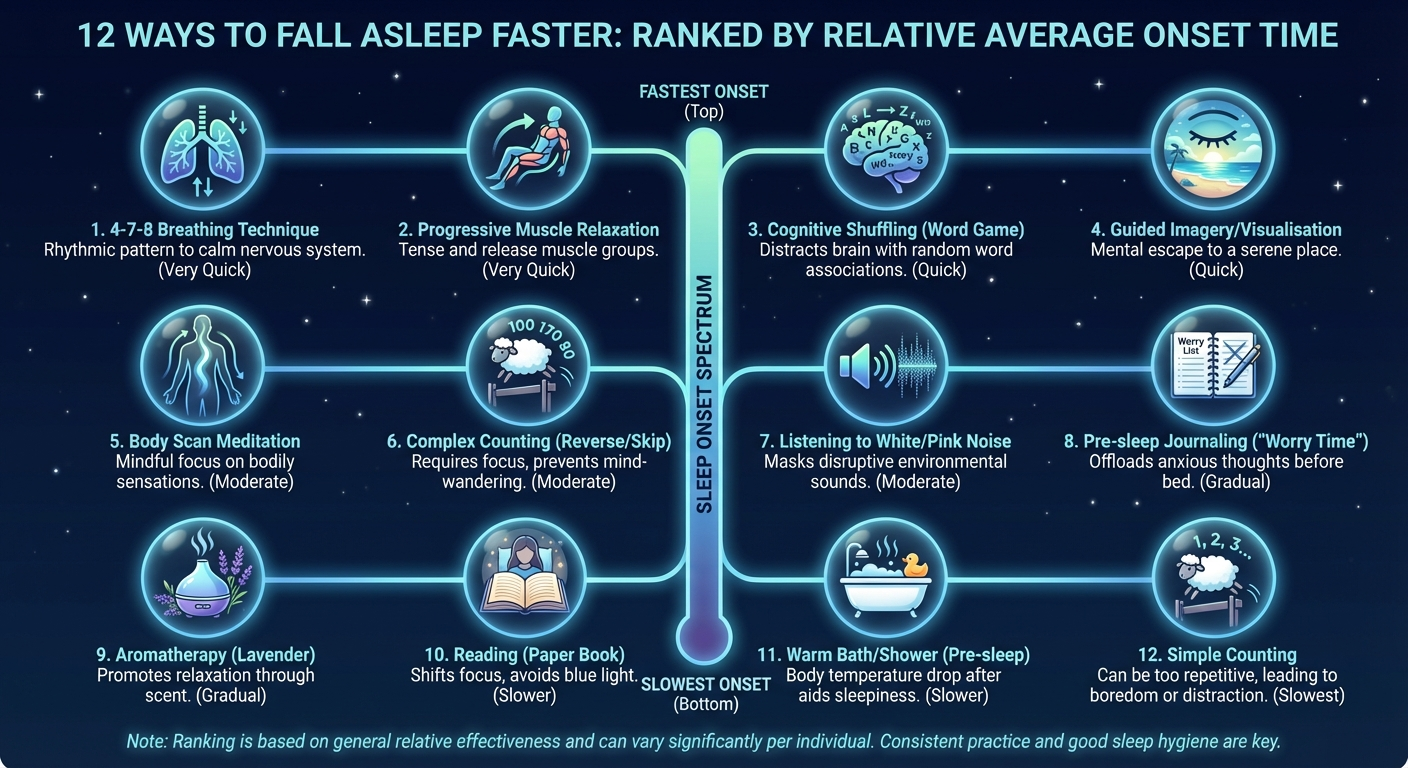 12 sleep onset techniques ranked by average time to sleep in clinical trials.
12 sleep onset techniques ranked by average time to sleep in clinical trials.
Technique 6: Paradoxical Intention
Targets: Sleep performance anxiety / emotional arousal Evidence level: Strong (included in AASM guidelines) Time to learn: Immediate
This technique sounds counterintuitive: instead of trying to fall asleep, you deliberately try to stay awake. But it's backed by rigorous evidence and is recommended by the American Academy of Sleep Medicine for treating insomnia.
How to Do It
- Lie in bed with the lights off.
- Keep your eyes open (gently, without straining).
- Tell yourself: "I'm going to try to stay awake as long as possible."
- Do not use any stimulation — no phone, book, or TV. Just lie there and try to stay awake passively.
- Allow sleep to come naturally, without effort.
Why It Works
Sleep is an involuntary process — you cannot force yourself to fall asleep any more than you can force yourself to digest food. When you try hard to sleep, you create performance anxiety, which triggers the stress response, which prevents sleep. This creates a vicious cycle that paradoxical intention breaks.
By removing the effort and pressure to sleep, you eliminate the anxiety-driven arousal that was keeping you awake. A 2003 randomized trial in Behavioural and Cognitive Psychotherapy found that paradoxical intention reduced sleep onset latency by 67% and was rated as "highly credible" by participants.
Technique 7: Body Scan Meditation
Targets: Physiological and cognitive arousal Evidence level: Moderate-Strong Time to learn: 1-2 weeks
Body scan meditation is a mindfulness-based technique that directs attention systematically through the body. Unlike PMR, you don't tense muscles — you simply observe sensations.
How to Do It
- Lie on your back with arms at your sides, palms up.
- Begin at the top of your head. Notice any sensations — warmth, tingling, pressure, or nothing at all.
- Slowly move your attention downward: forehead → eyes → cheeks → jaw → neck → shoulders → each arm to fingertips → chest → abdomen → hips → each leg to toes.
- Spend 20-30 seconds with each area.
- If your mind wanders, gently redirect attention back to the body part you were observing. Wandering is not a failure — it's a normal part of the process.
A 2015 randomized trial published in JAMA Internal Medicine found that mindfulness meditation (including body scan) improved sleep quality scores significantly more than a structured sleep hygiene education program. Participants showed improvements in insomnia severity, fatigue, and depression.
 Offloading anxious thoughts to paper prevents the mental replay loop that keeps you awake.
Offloading anxious thoughts to paper prevents the mental replay loop that keeps you awake.
Technique 8: The Cool-Down Method
Targets: Physiological arousal (thermoregulation) Evidence level: Strong Time to learn: Immediate
Your core body temperature must drop by approximately 1-2°F to initiate and maintain sleep. You can strategically accelerate this process.
How to Do It
- Take a warm bath or shower 1-2 hours before bed (water temperature 104-109°F / 40-42.5°C, duration 10+ minutes). This sounds counterintuitive, but the warm water dilates blood vessels at the skin's surface. After you exit, the rapid heat dissipation drops your core temperature significantly.
- Keep your bedroom cool — 60-67°F (15.5-19.4°C).
- Consider cooling accessories — a cooling pillow, breathable sheets, or keeping your feet outside the covers (feet are highly vascularized and radiate heat effectively).
A 2019 systematic review in Sleep Medicine Reviews analyzing 5,322 studies found that a warm bath 1-2 hours before bed reduced sleep onset latency by an average of 36% (approximately 10 minutes faster). The optimal timing was 1-2 hours before bed, allowing the post-bath temperature drop to coincide with bedtime.
Technique 9: Guided Imagery and Visualization
Targets: Cognitive and emotional arousal Evidence level: Moderate Time to learn: Immediate
Research from Oxford University, published in Behaviour Research and Therapy (2002), compared three pre-sleep strategies: imagery distraction (visualizing a calming scene), general distraction (counting sheep), and no instructions. The imagery group fell asleep 20 minutes faster than both other groups.
How to Do It
- Choose a detailed, calming scenario — a forest path, a quiet beach, floating on a calm lake, or walking through a peaceful garden.
- Engage all five senses in the visualization:
- See the details: colors, light, textures
- Hear the sounds: waves, birdsong, rustling leaves
- Feel the sensations: warmth of sunlight, cool breeze, soft sand
- Smell the environment: ocean air, pine trees, flowers
- Taste if applicable: salt spray, fresh air
- Explore the scene slowly and thoroughly. Do not rush.
- If thoughts intrude, gently return to the scene.
Why it works better than counting sheep: Counting sheep is too simple to occupy working memory — intrusive thoughts easily break through. A rich, multi-sensory visualization fully engages the cognitive resources that would otherwise generate worry and rumination.
 White noise masks environmental sounds that would otherwise trigger micro-arousals.
White noise masks environmental sounds that would otherwise trigger micro-arousals.
Technique 10: Sleep Restriction Therapy
Targets: Insufficient sleep drive / conditioned wakefulness Evidence level: Strong (core CBT-I component) Time to learn: 2-6 weeks
Important: This technique should ideally be supervised by a clinician, particularly if you have conditions like epilepsy, bipolar disorder, or a job requiring high alertness (driving, operating machinery).
Sleep restriction therapy, developed by Arthur Spielman, works by temporarily limiting time in bed to match actual sleep time, thereby consolidating sleep and increasing sleep drive.
How to Do It
- Track your sleep for 1-2 weeks using a sleep diary. Calculate your average total sleep time (TST).
- Set your time in bed (TIB) to equal your TST, with a minimum of 5.5 hours. For example, if you average 6 hours of actual sleep despite being in bed for 8 hours, set your sleep window to 6 hours.
- Choose a fixed wake time (e.g., 6:30 AM) and count backward to determine your bedtime (e.g., 12:30 AM).
- Do not go to bed before your scheduled bedtime, no matter how sleepy you feel.
- When your sleep efficiency (TST ÷ TIB × 100) reaches 85% or higher for 5 consecutive days, add 15 minutes to your sleep window by going to bed 15 minutes earlier.
- Repeat until you reach an optimal sleep duration with maintained efficiency.
A 2014 meta-analysis in Annals of Internal Medicine found that sleep restriction, as part of CBT-I, produced durable improvements in sleep onset latency, wake after sleep onset, and sleep efficiency that persisted for at least 12 months after treatment ended.
Technique 11: Strategic Light Management
Targets: Circadian misalignment Evidence level: Strong Time to learn: 1-2 weeks for circadian adjustment
If you're a "night owl" struggling to fall asleep at a conventional bedtime, your circadian rhythm may simply be delayed. Strategic light exposure can shift your internal clock earlier.
How to Do It
- Morning bright light exposure: Get 30-60 minutes of bright light (10,000 lux light therapy box or outdoor sunlight) within 30 minutes of your desired wake time.
- Evening light restriction: Dim all lights to below 50 lux starting 2-3 hours before bed. Switch to amber/red-tinted lighting. Wear blue-light-blocking glasses if using screens.
- Maintain consistency: Your circadian clock shifts by approximately 1-2 hours per week with consistent light management. If your sleep is delayed by 2 hours, expect 1-2 weeks to see the full adjustment.
A 2020 study in Sleep Medicine found that a combination of morning bright light therapy and evening blue-light-blocking glasses advanced circadian timing by 80 minutes and reduced sleep onset latency by 50% in participants with delayed sleep-wake phase disorder.
 A cool shower triggers the body temperature drop that initiates sleep onset.
A cool shower triggers the body temperature drop that initiates sleep onset.
Technique 12: The Pre-Sleep Cognitive Offload
Targets: Cognitive arousal Evidence level: Moderate Time to learn: Immediate
Research from Baylor University published in the Journal of Experimental Psychology: General (2018) tested a simple but powerful intervention: writing a to-do list before bed.
How to Do It
- Set aside 5-10 minutes before your wind-down routine (ideally 1-2 hours before bed).
- Write a detailed to-do list for the next day and the rest of the week. Be specific — not "work on project" but "draft introduction for quarterly report; email Sarah about budget figures."
- Write down any unresolved worries and, if possible, a single next action step for each.
- Close the notebook and set it aside. The physical act of closing the book signals that these concerns are captured and can be addressed tomorrow.
Participants who wrote specific to-do lists fell asleep 9 minutes faster than those who wrote about completed tasks or didn't write at all. The more specific the list, the faster participants fell asleep — suggesting that the act of offloading cognitive "open loops" reduces the mental rumination that delays sleep.
Combine this with a comprehensive sleep hygiene routine for maximum effect — see .
Technique Comparison Table
| Technique | Primary Target | Evidence Level | Avg. Improvement | Best For | Difficulty |
|---|---|---|---|---|---|
| Military Sleep Method | Physiological + cognitive | Moderate | Varies | General sleep onset difficulty | Medium |
| Progressive Muscle Relaxation | Physiological | Strong | 20-30% faster onset | Physical tension, muscle tightness | Easy |
| 4-7-8 Breathing | Physiological + emotional | Moderate | 15-25% faster onset | Anxiety, racing heart at bedtime | Easy |
| Cognitive Shuffling | Cognitive | Moderate | 30-40% faster onset | Racing thoughts, overthinking | Easy |
| Stimulus Control | Conditioned wakefulness | Strong | 40-60% faster onset | Chronic insomnia, bed = wakefulness | Hard (initially) |
| Paradoxical Intention | Sleep anxiety | Strong | 50-67% faster onset | Performance anxiety about sleep | Easy |
| Body Scan Meditation | Physiological + cognitive | Moderate-Strong | 20-30% faster onset | General tension and restlessness | Easy |
| Cool-Down Method | Thermoregulation | Strong | 36% faster onset | Overheating, physiological arousal | Easy |
| Guided Imagery | Cognitive + emotional | Moderate | 20 min faster onset | Worry, rumination | Easy |
| Sleep Restriction | Sleep drive | Strong | 40-60% faster onset | Chronic insomnia (with guidance) | Hard |
| Strategic Light Management | Circadian misalignment | Strong | 50% faster onset | Night owls, delayed sleep phase | Medium |
| Pre-Sleep Cognitive Offload | Cognitive | Moderate | 9 min faster onset | Worry about tasks, "open loops" | Easy |
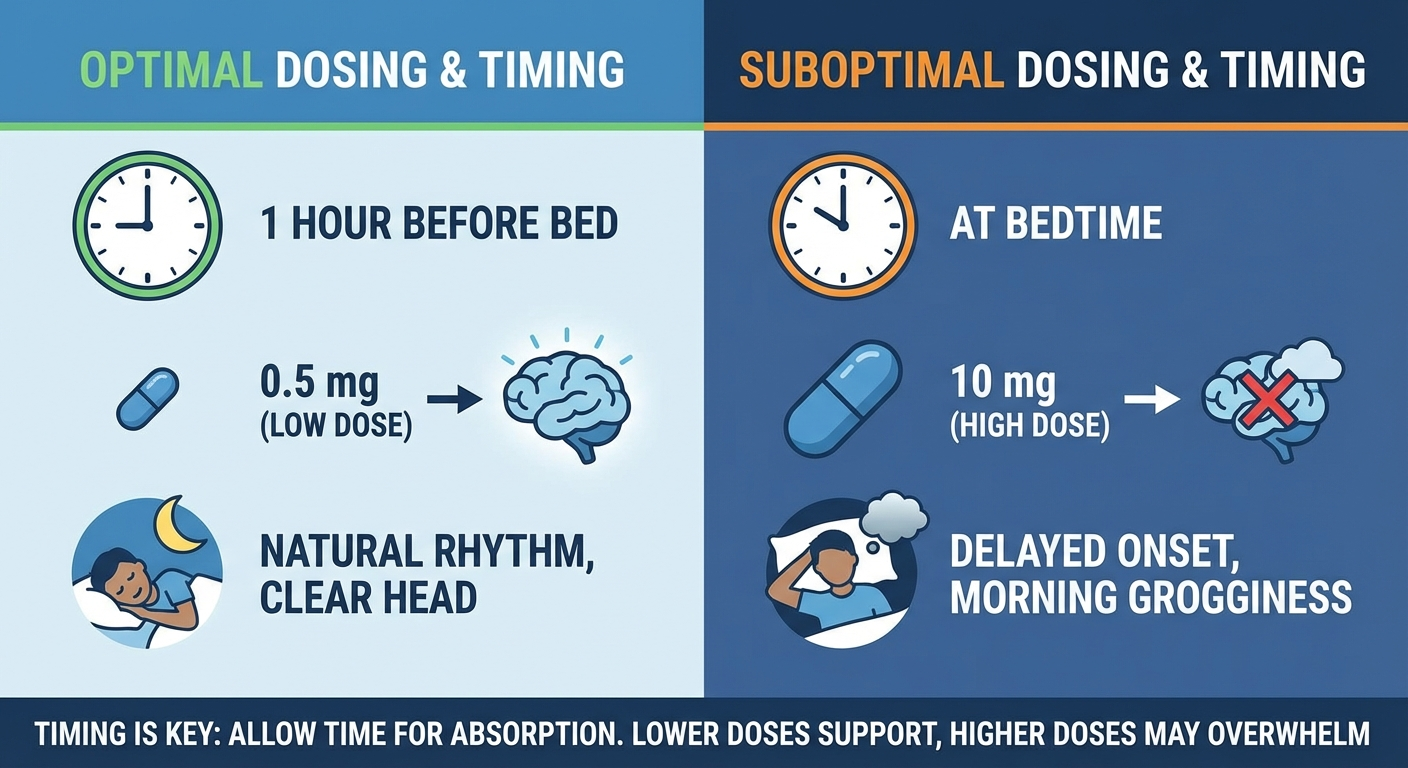 Most people take 10-20x the effective melatonin dose — 0.5mg works better, not 10mg.
Most people take 10-20x the effective melatonin dose — 0.5mg works better, not 10mg.
Building Your Personal Sleep Onset Protocol
You don't need all 12 techniques. Based on your primary sleep onset problem, here are recommended combinations:
If your main problem is racing thoughts:
- Pre-Sleep Cognitive Offload (evening)
- Cognitive Shuffling (in bed)
- Stimulus Control (if thoughts persist beyond 20 minutes)
If your main problem is physical tension or restlessness:
- Cool-Down Method (1-2 hours before bed)
- Progressive Muscle Relaxation (in bed)
- 4-7-8 Breathing (between PMR cycles)
If your main problem is anxiety about sleeping:
- Paradoxical Intention (primary technique)
- 4-7-8 Breathing (to reduce physiological anxiety)
- Body Scan Meditation (alternative for nights when anxiety is lower)
If your main problem is being a night owl:
- Strategic Light Management (ongoing daily practice)
- Cool-Down Method (to support temperature drop)
- Military Sleep Method or PMR (in bed)
If you have chronic insomnia:
- Stimulus Control + Sleep Restriction (core CBT-I, ideally clinician-guided)
- Cognitive Shuffling or Paradoxical Intention (supplementary)
- Pre-Sleep Cognitive Offload (evening routine)
For supplements that may support these techniques, see .
When Techniques Aren't Enough: Red Flags
Self-help techniques are powerful, but some situations require professional evaluation. Seek help if:
- You've consistently applied techniques for 6+ weeks without improvement
- You experience excessive daytime sleepiness that impairs daily functioning or safety (especially driving)
- Your partner reports loud snoring, gasping, or breathing pauses during sleep
- You have restless, uncomfortable, or creeping sensations in your legs at bedtime
- You experience sleepwalking, acting out dreams, or unusual nighttime behaviors
- Your sleep difficulties began after starting a new medication
- You have untreated anxiety, depression, or PTSD — these conditions frequently cause insomnia and require specific treatment
Cognitive Behavioral Therapy for Insomnia (CBT-I) delivered by a trained therapist remains the gold standard treatment for chronic insomnia, with durable effects that outlast sleep medications. Ask your physician for a referral, or look for CBT-I providers through the Society of Behavioral Sleep Medicine directory.
FAQ
How long should it take to fall asleep?
A healthy sleep onset latency is between 10 and 20 minutes. Falling asleep in under 5 minutes may indicate sleep deprivation, while consistently taking longer than 30 minutes suggests a sleep onset difficulty that may benefit from clinical evaluation.
Why can't I fall asleep even when I'm tired?
This paradox is usually caused by hyperarousal — your body is tired but your nervous system is still activated. Common causes include anxiety, stress, excessive screen use, caffeine consumed too late, or conditioned wakefulness from spending too much time awake in bed. Techniques like cognitive shuffling and progressive muscle relaxation specifically target this arousal.
Does the military sleep method really work?
The military sleep method, which involves systematically relaxing your face, shoulders, arms, and legs while clearing your mind, is a structured relaxation technique. While no peer-reviewed study has specifically tested the military method by name, it combines progressive muscle relaxation and autogenic training, both of which have strong clinical evidence for reducing sleep onset latency.
Is it better to stay in bed or get up if I can't sleep?
If you have been lying awake for more than 20 minutes, get up and go to a different room. Engage in a quiet, low-stimulation activity in dim light until you feel sleepy, then return to bed. This technique, called stimulus control, prevents your brain from associating the bed with wakefulness and is one of the most effective components of CBT-I.
Can supplements help me fall asleep faster?
Some supplements have evidence for reducing sleep onset latency. Melatonin (0.5 to 3 mg taken 30 to 60 minutes before bed) is the most studied and can reduce sleep onset time by 7 to 12 minutes on average. Magnesium glycinate and L-theanine also show promise. However, supplements should complement, not replace, good sleep hygiene practices. See our full guide: .
Does counting sheep actually work?
Research from Oxford University found that counting sheep was actually less effective than imagery distraction for falling asleep. Participants who visualized a calming scene like a beach or waterfall fell asleep 20 minutes faster than those who counted sheep. The reason is that counting sheep is too boring to hold attention, allowing intrusive thoughts to return.
What is sleep anxiety and how do I stop it?
Sleep anxiety, also called somniphobia or sleep performance anxiety, is the fear of not being able to fall asleep. Paradoxically, this anxiety activates the fight-or-flight response, making sleep even harder. The most effective approach is paradoxical intention — deliberately trying to stay awake — which removes the performance pressure and allows sleep to occur naturally.
Sources and Methodology
This article synthesizes findings from peer-reviewed research, clinical guidelines, and expert consensus. Key sources include:
- Riemann, D., et al. (2010). "The hyperarousal model of insomnia: A review of the concept and its evidence." Sleep Medicine Reviews, 14(1), 19-31.
- Liu, Y., et al. (2020). "Progressive muscle relaxation for sleep quality: A systematic review and meta-analysis." BMC Complementary Medicine and Therapies, 20, 302.
- Beaudoin, L.P., et al. (2020). "Cognitive shuffling and sleep onset." Behaviour Research and Therapy, 126, 103561.
- Broomfield, N.M., & Espie, C.A. (2003). "Paradoxical intention for insomnia: A randomized controlled trial." Behavioural and Cognitive Psychotherapy, 31(3), 313-324.
- Haghayegh, S., et al. (2019). "Before-bedtime passive body heating by warm shower or bath to improve sleep." Sleep Medicine Reviews, 46, 124-135.
- Harvey, A.G., & Payne, S. (2002). "The management of unwanted pre-sleep thoughts in insomnia: Distraction with imagery versus general distraction." Behaviour Research and Therapy, 40(3), 267-277.
- Scullin, M.K., et al. (2018). "The effects of bedtime writing on difficulty falling asleep." Journal of Experimental Psychology: General, 147(1), 139-146.
- Black, D.S., et al. (2015). "Mindfulness meditation and improvement in sleep quality." JAMA Internal Medicine, 175(4), 494-501.
- Bootzin, R.R., & Epstein, D.R. (2011). "Understanding and treating insomnia." Annual Review of Clinical Psychology, 7, 435-458.
- Trauer, J.M., et al. (2015). "Cognitive behavioral therapy for chronic insomnia: A systematic review and meta-analysis." Annals of Internal Medicine, 163(3), 191-204.
- Veqar, Z., & Hussain, M.E. (2020). "Strategic light therapy and circadian phase advancement." Sleep Medicine, 75, 411-418.
- Jerath, R., et al. (2019). "Physiology of slow breathing and cardiovascular implications." Physiological Reports, 7(2), e14019.
- American Academy of Sleep Medicine. (2025). Clinical Practice Guidelines for Behavioral Treatment of Insomnia. aasm.org.
Methodology: Techniques are ranked by evidence level based on the quality and quantity of supporting research. "Strong" indicates support from multiple RCTs and/or meta-analyses. "Moderate" indicates support from at least one RCT or multiple observational studies. Improvement estimates are drawn from published effect sizes and should be interpreted as population averages — individual results will vary.
Medical Disclaimer: This article is for informational purposes only and does not constitute medical advice. The techniques described here are based on published research and clinical guidelines but should not replace professional medical consultation. Sleep restriction therapy in particular should be supervised by a clinician in individuals with certain medical conditions. If you have a sleep disorder, chronic insomnia, or a medical condition affecting your sleep, consult a qualified healthcare provider. Dr. Nicole Chambers is a sleep medicine specialist and clinical psychologist. Individual results may vary.
Written by Dr. Nicole Chambers, Sleep Medicine Specialist & Clinical Psychologist — Sleep Better Faster © 2026